
Understanding Carpal tunnel syndrome – Leigh Johnson, PURE Sports Medicine physiotherapist, gives us the lowdown on carpal tunnel syndrome.
Carpal tunnel syndrome (CTS) is any pressure on the anatomical tunnel located at the palmer side of our wrists. This is made of bones and a fibrous band called the flexor retinaculum. This contains nine tendons and a branch of the median nerve, one of the main peripheral nerves supplying the palm and the first 3.5 fingers.1 Due to the tunnel’s non-extendable structure, it is not very accommodating to increased pressure such as swelling or compression of the wrist.2,3 This is when CTS can present.
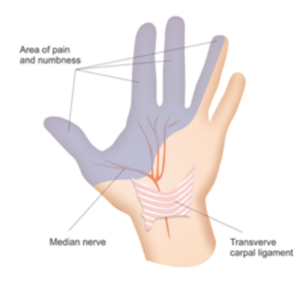
Photo courtesy of: https://hempsteadtherapycentre.co.uk/carpal-tunnel-syndrome/
CTS is one of the most common nerve entrapments, with some studies suggesting that 3% of the general population experience symptoms and for those in occupations involving forceful and repetitive hand tasks the prevalence is between 5-15% 4
Presentation
Those with CTS may complain of symptoms such as:
- numbness or pins and needles of the first 3.5 digits and nail beds
- pain may be described as ‘burning’ or ‘shooting’ and is often worse at night-time
- relief when shaking their hands
- loss of grip strength
- struggling with fiddly tasks such as buttons.5
As one of the more well-known hand conditions, it can often be over diagnosed. For that reason, it is helpful to understand symptoms that are not often associated with CTS:
- Symptoms anywhere other than in the first 3.5 digits
- Numbness or pins and needles on the entire palm or whole hand
- Pain or sensation changes above the wrist6
The wrist is only one junction of possible entrapment of the median nerve. The nerve originates from the neck, where it travels down crossing through and under numerous anatomical structures, posing numerous potential risks of entrapment. Symptoms described above are associated with CTS only and therefore symptoms outside of these could indicate a lesion elsewhere.7 This would need a formal assessment from a healthcare professional.
Those at risk
As mentioned, compression and repetitive use of the hands increase risk of swelling and narrowing of the carpal tunnel. There are also links to medical causes which will predispose them to CTS:
- Diabetes
- Pregnancy
- Underactive thyroid
- Trauma, such as broken wrist bones or sprains
- Osteo or rheumatoid arthritis
- Obesity8
Treatment
Treatment varies, depending on the severity and stage of recovery. Those with symptoms must be reviewed by a therapist who will offer appropriate management. The following points are some considerations for their recovery.
Bracing
Wrist bracing is an effective treatment modality. Braces should maintain a neutral position, blocking wrist movement and leaving fingers to move freely. This prevents compression caused by repetitive movement at the wrist, subsequently allowing irritation and swelling to settle, restoring normal pressure within the tunnel and nerve supply to the hand.9 Clients can buy a comfortable splint over the counter/online. Alternatively, they can be moulded to the individual’s wrist by a trained therapist using thermoplastic.
They will be advised to use braces during aggravating tasks like housework or gym work and at night to avoid sustained bending in curled-up positions for four to eight weeks or until the symptoms settle11.
Getting back to the gym
There is no conclusive data that suggests that weightlifting and gym-based exercise will cause CTS. That said, if someone is experiencing CTS, there are things that may aggravate these symptoms during their rehab.
Communication
CTS pain does not always present at the time of the aggravator. Pain often presents later and sometimes the next day. Therefore, when introducing clients back into the gym, remember to start with lighter weights and with lower reps and larger rest times. It is vital to ensure clients monitor their symptoms over the next 24 hours. You can use this feedback to gauge the appropriateness to progress or regress.
Wrist posture
Higher loads will correlate with larger gripping forces which, again, increases carpal tunnel pressure12. This is when grip strength and ‘wrist posture’ should be considered13. Regaining grip strength throughout and after CTS is imperative not only for daily function but can also help reduce their symptoms14. Gradual exposure to pulling exercises like rows, suitcase carries, deadlifts and pull-up variations will secondarily use and train grip strength, which I think is a lot more fun than squeezing stress balls and grip trainers!15
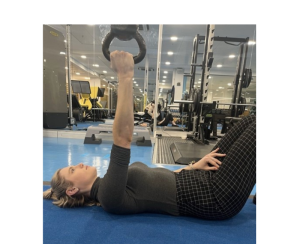
Improved grip strength can help clients progress safely to pushing-based exercises. Try to maintain a stacked position during vertical lifts, keeping a neutral mid position at the wrist joint. Think ‘punching the ceiling’. Certain exercises can help with training stability within this range, for example, a bottom-up kettlebell press where the client must balance the bell above the fist through range.

Activity modification
Loaded wrist extension can also aggravate CTS, such as in high planks or push-ups. A ‘fist’ push-up modification can help and is quick and easy16 but I often suggest clients grip something small and soft in their hands, such as a small gym towel, during these motions to take pressure off their knuckles. Other alternatives to reduce wrist extension are a folded towel or rolled mat under the heel of the hand or using a step to reduce extension angle. Again, I would advise taking breaks between holds and building up durations gradually.


Nerve glides
After a formal diagnosis of CTS, clients are often advised to try a variation of a nerve glide exercise shown below. The client’s shoulder and elbow are bent to 90˚, palm facing forward. Level 1 involves opening and closing their fingers. Level 2 involves extending the elbow out straight and/or tilting the head away from the affected side. This can cause delayed irritation, so I would suggest they start level one for 30 seconds three times a day and progress slowly over time, unless guided by their healthcare provider.17


General wellbeing
As always, general health and wellbeing is imperative. Factors such as optimised sleep, mental health, stress and diet can all play a role in recovery18. Make sure clients are aware of this and support them in optimising lifestyle choices when able.
Medical intervention
If symptoms persist, clients with CTS should discuss with a healthcare professional about their alternative avenues to recovery if conservative management has failed. These can include injections or surgical interventions, which will have their corresponding recovery times.19
To summarise, CTS is a common and uncomfortable condition to manage; however, it is entirely possible to still maintain physical activity! Communicate openly with the client about their specific medical advice, symptoms and triggers and guide them to gradually achieve their goals. When in doubt, there is always the option for extra leg day!

Leigh Johnson
Leigh Johnson has experience in treating a range of musculoskeletal pathologies throughout the body and a special interest in the upper limb, particularly the hand and wrist. She most enjoys treating wrist instability, ligament injuries, thumb pain and helping people return to sport following surgery. Over the last seven years she has gained valuable experience treating conditions ranging from traumatic injuries to repetitive loading injuries.
Read more about nerves, injury and rehab in this FitPro blog post
- Carpal Tunnel Syndrome Justin O. Sevy; Matthew Varacallo. Last Update: December 21, 2019. Available from:https://www.ncbi.nlm.nih.gov/books/NBK448179/ (last accessed 22.3.2020)
- Carpal Tunnel Syndrome Justin O. Sevy; Matthew Varacallo. Last Update: December 21, 2019. Available from:https://www.ncbi.nlm.nih.gov/books/NBK448179/
- https://hempsteadtherapycentre.co.uk/carpal-tunnel-syndrome/
- Neal, S., & Fields, K. B. (2010). Peripheral nerve entrapment and injury in the upper extremity.[Review]. Am Fam Physician, 81(2), 147-155.
- Ashworth NL, MBChB. Carpal Tunnel Syndrome Clinical Presentation [Internet]. 1994 [Updated 2014 Aug 25; cited 2015 March 20].fckLRAvailable from:fckLRhttp://emedicine.medscape.com/article/327330-clinical.
- Hobson‐Webb, L. D., Padua, L., Martinoli, C., Bianchi, S., Gandolfo, N., Valle, M., et al. (2012). Ultrasonography in the diagnosis of peripheral nerve disease. Expert Opinion on Medical Diagnostics, 6(5), 457-471.
- Toussaint CP, Perry EC 3rd, Pisansky MT, Anderson DE. What’s new in the diagnosis and treatment of peripheral nerve entrapment neuropathies. Neurol Clin. 2010 Nov;28(4):979-1004. doi: 10.1016/j.ncl.2010.03.017. PMID: 20816274.
- Carpal Tunnel Syndrome Justin O. Sevy; Matthew Varacallo. Last Update: December 21, 2019. Available from:https://www.ncbi.nlm.nih.gov/books/NBK448179/ (last accessed 22.3.2020)
- Page MJ, Massy-Westropp N, O’Connor D, Pitt V. Splinting for carpal tunnel syndrome.
- Google images
- Golriz B, Ahmadi Bani M, Arazpour M, Bahramizadeh M, Curran S, Madani SP, et al.. Comparison of the efficacy of a neutral wrist splint and a wrist splint incorporating a lumbrical unit for the treatment of patients with carpal tunnel syndrome. Prosthet Orthot Int 2016; 40: 617-623
- Chen N et al. Prevalence status and associated factors of wrist postural injury in the Chinese occupational population. Front Public Health. 2022;10:1047814. Published online 2022 Nov 23. doi: 10.3389/fpubh.2022.1047814. PMCID: PMC9727286. PMID: 36504943.
- The Physician and Sportsmedicine. 2005 Jul;33(7):24-37. Peripheral Nerve Injuries in Weight Training: Sites, Pathophysiology, Diagnosis, and Treatment. DOI: 10.3810/psm.2005.07.141
- Michlovitz SL. Conservative interventions for carpal tunnel syndrome. J Orthop Sports Phys Ther. 2004 Oct;34(10):589-600. doi: 10.2519/jospt.2004.34.10.589. PMID: 15552705.
- Borges, Iñigo & González Fernández, Francisco Tomás & Rico-González, Markel. (2022). The influence of deadlift and an additional training programme on grip strength in trained subjects: an experimental study. Revista Andaluza de Medicina del Deporte. 15. 86-92. 10.33155/j.ramd.2022.07.001
- Polovinets, Olga & Wolf, Alon & Wollstein, Ronit. (2017). Force transmission through the wrist during performance of push-ups on a hyperextended and a neutral wrist. Journal of Hand Therapy. 31. 10.1016/j.jht.2017.04.005.
- Meng S, Reissig L.F., Beikircher R, Tzou C. H., Grisold W, Weninger W.J. (2015). Longitudinal gliding of the median nerve in the carpal tunnel: Ultrasound cadaveric evaluation of conventional and novel concepts of nerve mobilization. Archives of physical medicine and rehabilitation 96 (12). doi: 10.1016/j.apmr.2015.08.415.
- Alsharif A, Al Habbal A, Daaboul Y, Al Hawat L, Al Habbal O, Kakaje A. Is psychological distress associated with carpal tunnel syndrome symptoms and nerve conduction study findings? A case-control study from Syria. Brain Behav. 2022 Feb;12(2):e2493. doi: 10.1002/brb3.2493. Epub 2022 Jan 18. PMID: 35040586; PMCID: PMC8865142.
- Bayramoglu, M. (2004). Entrapment neuropathies of the upper extremity. Neuroanatomy, 3(1), 18-24.




