
Justin Price offers exercises to help prevent tennis injuries, so you can help clients to knock tennis pain out of the park.
Recent polls show that tennis is one of the most prevalent sports in the world, with over 87 million people participating and predictions that number will increase to nearly 120 million by 2030.1 Being such a popular activity, it is likely that you have both current clients and prospective customers who need your help preparing their body for tennis. Unfortunately, people who play tennis are susceptible to injury due to its dynamic nature and forceful twisting motions.2 Therefore, as a fitness professional working with people who play or are interested in playing tennis, it is your job to understand what causes these injuries and address the underlying causes so clients can enjoy this activity for many years to come without the risk of pain and injury.
Tennis injuries
The most common tennis injuries are joint and muscle strains to the knees, lower back and shoulders.2 To appreciate what causes these types of injuries, you first need to understand some basic tennis biomechanics.
Performing groundstrokes successfully in tennis (i.e., a forehand or backhand) requires the body to generate a lot of power to hit the ball. This force is achieved in large part by taking the racket back and following through quickly as the ball is struck. To facilitate this action, the leg must pivot in the hip socket to enable the spine and shoulders to rotate and the arms to swing (Figure 1).2

Figure 1: The leg pivots in the hip during the backswing and follow through
To generate even more power, advanced tennis players will often jump off the ground as they complete their backswing and follow through. These movements also occur in conjunction with the pivoting of the leg/hip to help generate rotation of the upper body (Figure 2).

Figure 2: Pivoting of leg in the hip facilitates powerful torso rotations
Ample hip rotation is necessary to hit forehands and backhands successfully, but also to mitigate stress to the areas of the body most commonly injured while playing tennis.2 The knees are a hinge joint designed primarily to flex and extend. The lumbar spine can rotate but not as effectively as the hips. The shoulder blades have the ability to protract and retract to assist with twisting movements of the torso, but similarly do not have the same rotational movement capabilities as the hips.3,4,5,6 Therefore, a lack of hip rotation can lead to overuse, pain and/or injury to the knees, lower back and shoulders when playing tennis.
Improving hip rotation
Improving a client’s ability to rotate their hips effectively is a three-step process:
- You must assess and make judgements about your client’s ability to both internally and externally rotate their hips.
- You must know how to identify which muscles and other soft tissue structures are affected by the movement restrictions you have identified.
- You must be skilled in selecting and designing appropriate corrective exercise strategies to address the muscle and movement dysfunction you have identified.3,4
Step 1: Assess internal and external hip rotation
The hip must have the capability to rotate both internally and externally in order for a person to perform tennis strokes well. Following are two assessments to enable you to evaluate hip rotation.
Internal hip rotation
Instruct the client to lie on the floor with legs spread about 18 to 24 inches apart. Coach them to try to turn both legs inward so their feet move towards each other (see Figure 3). Tell them not to bend the knees or let the pelvis lift off the ground as they rotate the legs inward. Now look to see how far they can turn their legs towards the midline. Both legs should be able to turn in about 40°. Assess if one leg cannot turn as far in as the other leg, or if both sides lack internal rotation. (Note: In the example below, the client has almost an acceptable range of motion for her left leg, while her right leg is severely lacking the mobility to rotate inward).

Figure 3: Assessing internal rotation
External hip rotation
Once you have completed the internal rotation assessment, instruct the client to try to turn both legs outward so their feet move away from each other (see Figure 4). Look to see how far they can turn their legs away from the midline. Again, remind them not to bend the knees or let the pelvis lift off the ground as they rotate the legs outward. Both legs should be able to turn out about 45°. Assess if one leg cannot turn as far out as the other leg, or if both sides lack external rotation. (Note: In the example below, the client has an acceptable range of motion for her right leg, while her left leg is lacking the mobility to rotate outward).

Figure 4: Assessing external rotation
Step 2: Identify affected soft tissue structures
If your assessment results reveal that a client lacks the ability to internally or externally rotate their hips, this may be indicative of the presence of problematic soft tissue and muscle imbalances.2
Hip rotation muscles
A thorough understanding of functional anatomy, and knowledge of those muscles that affect hip function, is imperative to help you choose the most appropriate corrective exercises to address a client’s condition. For example, an inability to internally rotate the hip may be due to muscle tightness and/or restrictions in the gluteus maximus, the posterior fibres of the gluteus minimus, tensor fascia latae and gluteus medius, the hip rotators, adductors, hip flexor group of muscles and obliques (indirectly). Conversely, an inability to externally rotate the hip may be due to soft tissue restrictions or dysfunction of the adductors, the anterior fibres of the tensor fascia latae, gluteus minimus and gluteus medius, hip rotators, the medial hamstring muscles and obliques (indirectly).3,4,5
In addition to the application of your anatomy knowledge, you can ask clients as they are performing the assessments to tell you where they feel the most tightness or restrictions. This will help guide you to the muscles and soft tissue structures that need addressing the most with corrective exercises.
Step 3: Choose appropriate corrective exercises
Once you have assessed your client’s ability to internally and externally rotate their hips, and decided which soft tissues and/or muscles have been affected by movement dysfunction, you can begin integrating corrective exercise strategies into their programme to improve their hip function, enhance their movement performance and decrease the incidence of pain and/or injury occurring when playing tennis.
Whether integrating corrective exercise strategies to improve internal or external hip rotation, you should begin with self-myofascial release (or self-massage) techniques to rejuvenate and regenerate dysfunctional soft-tissue structures and muscles before stretching and then strengthening exercises are introduced.3,4,7,8
Improving internal rotation
Use equipment such as foam rollers to address larger areas and entire muscle groups that might be affecting your client’s ability to internally rotate their hip (e.g., gluteus maximus and adductors). Utilise massage balls (e.g., tennis balls) with a smaller surface area to address more specific areas of muscle dysfunction (i.e., the posterior fibres of the abductors, tensor fascia latae, origin of hip flexor group, hip rotators, etc.) (see Figure 5 for an example).3,4,9 Asking a client for feedback on tender areas when performing self-myofascial release exercises can also help direct you to specific structures that need addressing to improve movement.

Figure 5: Tennis ball on hip rotators
(Coach clients to pause on any sore spots for five to 10 seconds until the tension releases and then move to another spot. Address all sore areas for total of two to three minutes on each side of the gluteal complex.)
Once the health and suppleness of your client’s muscles have been restored, begin introducing stretching exercises to increase the flexibility of those muscles needed to facilitate better internal rotation of the hip. Start their stretching programme with isolated stretches of the gluteus maximus, abductors, hip flexors, adductors, tensor fascia latae and hip rotators (see Figure 6 for an example).

Figure 6: Isolated abductor stretch
(Coach clients to drop their knee toward the midline and use the weight of their other leg to increase the stretch. Instruct them not to arch their back or raise their pelvis off the ground as they drop their knee toward the midline.)
As the flexibility of individual soft-tissue structures increases, incorporate more dynamic forms of stretching that introduce multiple parts of the body that mimic tennis-specific movements (see Figure 7 for an example).

Figure 7: Wall rotation stretch
(This exercise resembles a backhand backswing in tennis for a right-handed player. It is designed to stretch the obliques, the hip flexors and adductors of the right leg, and the entire gluteal complex of the left leg. Coach the client to rotate over their front leg, utilising the wall to increase the rotation of their torso. Pay special attention to ensure the client does not arch their lower back excessively or lean to one side as they perform this stretch.)
As the desired range of internal hip rotation is achieved, you can begin integrating strengthening exercises that eccentrically load (i.e., lengthen under tension) the appropriate structures with the feet on the ground (i.e., closed kinetic chain exercises).
Utilise exercises that internally rotate the leg by pivoting the torso around the weight-bearing side. Perform movements where the hip is either flexed (i.e., with the knee bent and the target leg/hip in front of the body) (see Figures 8 and 9 for examples) or extended (i.e., with the target leg/hip straight and/or behind the body) (see Figure 10 for an example).

Figure 8: Lunge with knee pull
(Coach the client to pull their front knee towards the midline to help increase internal rotation and abduction of their hip/leg. Progress exercise by instructing them to rotate their torso away from the front leg [i.e., similar to what might happen during a follow through of a backhand in tennis].)

Figure 9: Single leg straight leg deadlift
(Coach the client to drop their left hip lower than their right hip to encourage more internal rotation and adduction of the weight-bearing leg.)

Figure 10: The pivot
(Coach the client to drop their left knee towards the midline as they tap their right foot on the ground for balance if needed. Instruct them to then extend their left leg and lift their right knee high to pivot around their left hip as much as possible.)
As your client’s movement capabilities improve, progress the strengthening phase of their programme by adding external loads to their exercises, such as instructing them to hold a medicine ball, a light weight and/or resistance bands.
Improving external rotation
If your assessment results reveal that a client lacks external rotation, utilise self-myofascial release techniques for their adductors, hamstring muscles toward the medial side of the leg (i.e., semitendinosus), the anterior fibres of their abductors (i.e., gluteus medius, gluteus minimus and tensor fascia latae) and their hip rotators.10 Progress when they are ready to isolated, and then integrated, stretching techniques that improve the range of motion of these muscles in preparation for the strengthening phase of their programme (see Figure 11 for an example).

Figure 11: Adductor stretch
(Example of isolated stretch for the adductor muscles. Progress to integrated stretches that incorporate more than one body part and also mimic real-life/tennis movements.)
As your client gains confidence and competence with increased ranges of motion, incorporate eccentric strengthening exercises to increase external rotation of their hip. Pivot the upper body around the leg/hip, utilising exercises where the foot of the weight-bearing leg is in contact with the ground (see Figure 12 for an example).
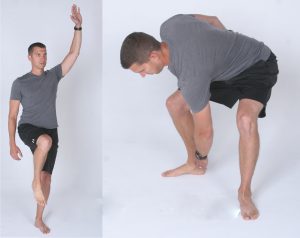
Figure 12: Sumo squat with rotation
(Coach the client to begin this exercise balanced on one leg in the pivot position as described in the pivot exercise provided previously. Instruct them to then rotate 45° away from their standing leg and squat before returning to the start position.)
As with all strengthening exercises, they can be progressed by adding external loads and/or uncontrollable variables such as coaching your client to catch and throw a ball as they perform the desired movement.
Conclusion
Effective internal and external rotation of the hip is important for improving tennis performance and decreasing pain/injury to the lower back, knees and/or shoulders during this dynamic sport. Hip rotation is also essential for producing power and minimising musculoskeletal stress during other sports that require forceful rotations of the trunk such as golf, throwing a baseball, throwing a discus/frisbee, etc. Therefore, the ability to assess and correct a client’s hip dysfunction rotation will not only help them to be more athletic on the tennis court, but also to enjoy their favorite sport(s) for longer and be less injury-prone as a result.
References
1. International Tennis Federation (2021), Participation Increases As ITF Publishes Global Tennis Report 2021. https://www.itftennis.com/en/news-and-media/articles/tennis-participation-increases-as-itf-publishes-new-data-in-the-itf-global-tennis-report-2021/ Retrieved 10 March 2023.
2. Kovacs M, Roetert P & Ellenbecker T (2016), Complete Conditioning for Tennis, 2nd ed. United States Tennis Association.
3. Price J & Bratcher M (2019), The BioMechanics Method Corrective Exercise Specialist Certification Program (2nd. Ed.), The BioMechanics Press.
4. Price J (2018), The BioMechanics Method for Corrective Exercise, Champaign, IL: Human Kinetics.
5. Cook G (2010), Movement, Aptos, CA: On Target Publications.
6. McGill S (2016), Low Back Disorders: Evidence-Based Prevention and Rehabilitation, 3rd ed. Champaign, IL: Human Kinetics.
7. Rolf IP (1989), Rolfing: Reestablishing the Natural Alignment and Structural Integration of the Human Body for Vitality and Well-Being, Rev ed. Rochester, VT: Healing Arts Press.
8. Myers TW (2008), Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists, 2nd ed. New York: Churchill Livingstone.
9. Price J (2013), The Amazing Tennis Ball Back Pain Cure, San Diego: The BioMechanics Press.
10. Gray H (1995), Gray’s Anatomy,New York: Barnes & Noble Books.






