
Dr Joanna Helcké PhD discusses postnatal return to exercise and her framework you can use for postnatal clients if perinatal fitness isn’t your specialism.
We get asked many questions by our clients and some of these are outside our remit – there’s something about working in the world of wellbeing that elicits medical questions. I feel strongly about knowing one’s skillset boundaries and understanding when it’s time to signpost people on. Indeed, being a fit pro with a wide range of professional connections one can refer people on to is, in itself, very beneficial for our clients and, in turn, helps build our credibility. As a specialist in perinatal fitness, I speak with feeling about inadvertently stepping beyond our field of expertise because, for many years, I’ve had to rectify fitness-related ‘advice’ offered by midwives, health visitors and GPs. I (we) get asked medical questions and they get asked fitness questions! I signpost on but they often provide inaccurate information.
Within our areas of expertise, it’s almost inevitable we’ll find ourselves with a client who has recently given birth and is asking for advice on returning safely to physical activity. You might get asked anything from “When can I rejoin my tug-of-war team?” to “When can I take up bungee fitness?” The variety is fantastic but, to answer these myriad questions, we need a framework on which to hang them. My aim is to provide a basic framework you can use for your postnatal clients if perinatal fitness isn’t your niche.
Strong foundations: The postnatal Tree of Fitness
Over years of giving talks on how to approach physical activity after childbirth, I have often used the analogy of a growing tree. You can have a tree with deep, strong roots that will grow tall and robust or a tree with shallow roots that may well soar upwards but without the vigour of the deep-rooted tree. At some point, the latter will have trouble withstanding the elements and may be uprooted or blown over. As everyday athletes, we need sturdy foundations, and this is even more relevant postpartum.
These strong roots lie largely hidden from view: I’m talking, of course, about our so-called core, which I visualise as a cylinder comprising the diaphragm at the top, the layers of abdominal and back muscles round our middle and the pelvic floor muscles at the base1. Unfortunately, out of sight often means out of mind until something starts to malfunction and, for women, certain bodily malfunctions have, until very recently, been dismissed as ‘normal’ – something you put up with. I am talking about pelvic floor dysfunction, for example, with symptoms such as urinary incontinence, urge incontinence or even pelvic organ prolapse (POP).
Our first – and crucial – job with postnatal clients is to assess the state of those ‘roots’ – their core – offer accurate information and correct any misinformation within the boundaries of being fitness professionals. In the first video, I go through how to check the abdominals postpartum, explaining what we are looking for, as well as what not to get too hung up on, and why. Many women have heard frightening things about ‘abdominal splits’ and it’s our role to allay worries by giving clients correct terminology and information that isn’t alarmist. I always explain in layman’s terms that there is no such thing as the abdominals ‘splitting’: the technical term for significant abdominal separation is diastasis recti (DR) and it’s not a tear in the muscle but a distancing of the left and right sides of the rectus abdominis muscles from the linea alba; this could be due to a weakening of the connective tissue or a deformation of the actual linea alba2. Look at the first video, which takes place in a home setting with baby on board – a reality that many, if not most, postpartum clients face when trying to exercise and rehab their bodies postpartum (another consideration when planning postnatal workouts and setting realistic targets …).
It’s my firm belief that all women should have an assessment with a women’s health physiotherapist (WHP) on the NHS. Unfortunately – unlike in France – this is not the case in the UK. If postnatal clients have the financial means, I suggest strongly advising them to have a full postnatal check-up with a private WHP3. This is an investment in their fitness future and will help proof them against injury down the line. You can direct them to the Mummy MOT4 which operates across the country and offers a full postnatal examination, including pelvic floor muscle assessment, which is something fitness professionals cannot do and MSK physios cannot perform either. Nevertheless, we can and should also ask pertinent questions regarding pelvic floor health since the pregnancy and birth, as the answers will give us strong clues on the next steps our clients should – and, crucially, should not – take. An example could be, “Have you, since the birth, had a go at switching your urine off mid-flow?” If the answer is that, yes, she has and she found it hard to do, then this is a strong indicator that a) the pelvic floor has been weakened and needs strengthening; b) that this should be taken into consideration when offering physical activity advice; and c) that she should see a WHP. At this point, I would suggest she asks her GP to refer her so she gets into the NHS system and, at the same time, she should consider going privately if at all possible.
Having checked the integrity of the abdominals, my next suggested step is to check whether the deeper layers of abdominal muscles – notably the transversus abdominal muscles (TVA) – automatically ‘fire up’ when required. An example of ‘when required’ could be a resisted move like raising your head and shoulders from the floor (the beginnings of a sit-up) or a cough, both of which create intra-abdominal pressure (IAP) the body must effectively manage. If the body does not ‘manage’ the IAP, this pressure will push through the weakest spot, which could be along the linea alba if your client has DR, could be the pelvic floor if these muscles have been weakened or could be fragile spots in the abdominals or diaphragm, with the potential to cause hernias in the longer term. In video two, I show the visual difference between an unguarded cough, where the deeper core muscles have not been activated, versus a cough after I have cued the TVA to be switched on. The difference is remarkable: hold on to this visual difference when planning a client’s postnatal return to physical activity.
The final part of the postnatal ‘strong roots’ approach is discussed in video three, where I give clients the necessary tools to figure out the correct level to work at: challenging enough to elicit progress without overstepping the mark, which can be counterproductive for abdominal rehabilitation. Giving postnatal clients the ability to judge how far they can push themselves is empowering for them and for you. Now you can give them a series of exercises to help rebuild core strength, which can safely be progressed over the weeks and months5.
The postnatal ‘tree of fitness’: Above ground
These initial assessment tools, alongside the expert feedback from a WHP (always ask for permission to have their feedback), will enable you to answer those varied questions and inform how you put together a logical, progressive plan to build back towards your client’s preferred form of fitness. Let’s take distance running/jogging as an example of a postpartum goal. She loves running, it helps her mental health, it’s ideal because she can run with her baby in a buggy and she can start her workout from her front door which saves time. That’s a lot of boxes ticked. However, “Running is a high-impact sport placing a lot of demand on the body. In a recent systematic review investigating urinary incontinence in female athletes, high-impact exercise was found to have a 4.59 fold increased risk of pelvic floor dysfunction compared to low-impact exercise …. We therefore recommend that a low-impact exercise timeline is followed within the first three months of the postnatal period, followed by a return to running between three and six months’ postnatal, at the earliest.”6
Being the bearer of unwelcome news is never easy but our aim is to successfully get our postnatal runner on board with the advice we are about to give. A bald “you mustn’t run for the next six months” is liable to be ignored unless framed constructively. Flipping this advice on its head, we can map out a plan of action so her end goal is in sight and achievable. Provide a bite-sized programme that will help rebuild her core and can be realistically fitted around early parenthood.
Here’s one example of how this could be articulated:
- “You plan to get back into marathon running – that’s such a great goal.
- “Your first step, now we’ve done the assessment of your abdominals and discussed pelvic floor, is to work on regaining those strong foundations: strengthening the core in a manner that challenges you without overstepping the mark. I’m going to give you a bite-sized programme you’ll be able to fit around daily life. Little and often is perfect. This is going to support your running later – and may eventually help you run better and faster.
- “Alongside this, you’ll be wanting to build up your stamina in a manner that won’t adversely affect your pelvic floor but will get you ready for running again at a later stage.
- “A good starting point – and easy to fit round busy mum-life – is power walking with your baby in a pram. Power walking is low impact and, if you maintain good form and a manageable speed, will keep you safe and challenged. Walking up hills can get your heart rate up – you could even do power walking hill reps. Walking with pace uphill with a pram is surprisingly hard work.
- “If you manage a little child-free time, spin classes are a great progression. Another excellent option is deep water aqua jogging, which translates to land once the time is right to pick up running.
- “When you are ready to test impact work, the NHS Couch to 5K programme is a great way to see how your body responds to gentle progression of impact exercise.”
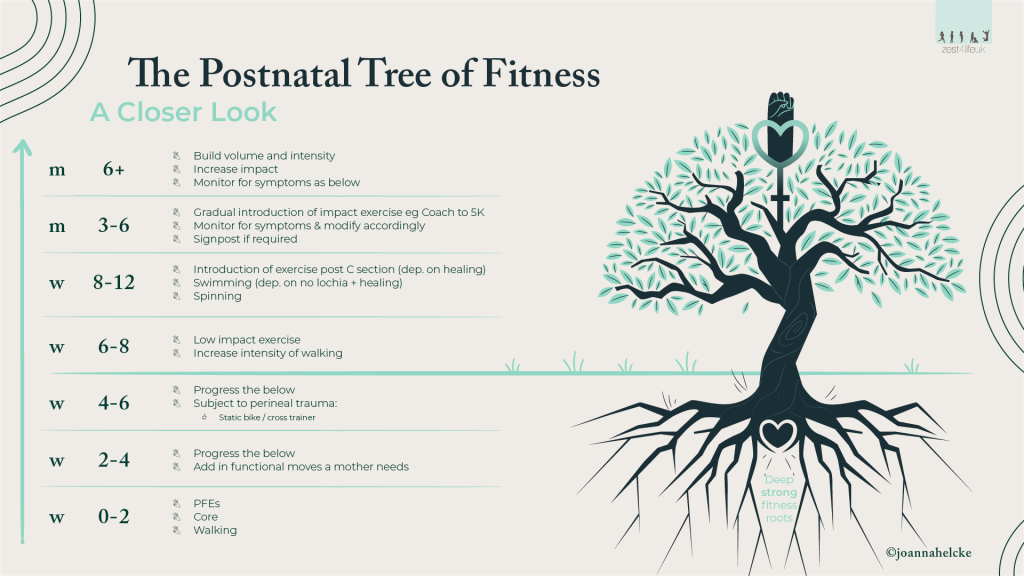
Take a look at the ‘Tree of Fitness’ image below, with the physical activity timeline for postnatal women, which you can use to safely move your clients towards their fitness goals.
Key is the importance of tailoring advice to the postpartum client’s fitness passion, so she’s more receptive to what might be unwelcome news about holding off from doing certain activities too soon. Asking an endurance athlete to take up weight training because it is low impact is liable to be as unwelcome a suggestion as telling a Crossfit enthusiast to take up aqua aerobics because it’s kind on the pelvic floor. This is where, in my view, we have to park our ideals, park our own fitness preferences (even if they are grounded in science) and suggest palatable stepping stones that will enable our clients to reach their goals safely. To this end, I have created a crib sheet, which you can download below, where I have tried to usefully group together different forms of fitness. It is by no means exhaustive but more of a logical framework you can use when asked slightly unusual questions, such as “When can I restart aerial silks?” Here is how to use the crib sheet:
- Each column aims to group together certain types of physical activity (e.g., high-impact exercise or resistance work). Clearly many forms of fitness cross these boundaries and one has to use one’s judgment.
- Working down each column, the next step gives you ‘things to watch out for’ such as diastasis recti (DR), pelvic organ prolapse (POP), symptoms of weak pelvic floor muscles, etc.
- Next, there is advice you can offer your client.
- And finally, as per the marathon runner example above, I give logical alternatives, designed to keep your client engaged in the process of pacing herself towards her longer-term goal.
Looking into the future
We are all passionate about seeing our clients reach their fitness goals, but not at the expense of ‘fitness longevity. Sometimes this involves imparting unwelcome advice and it is our role to explain this in a manner that will be greeted by acceptance. We need to ‘sell the boring stuff’ to them: the reality is that a perfectly toned pelvic floor isn’t as gratifying as the visual feedback of a sculpted six-pack! But weak pelvic floor muscles – or, even worse, POP – will halt clients in their tracks. One only has to go to a group fitness class and look around at the women doing single-leg jacks rather than jumping jacks. I can assure you it’s not a lack of stamina stopping them from performing jumping jacks: it’s weak pelvic floor muscles. How frustrating for them. Our job is to win them over and feed those deep roots so they may grow tall and strong right into old age. The future of health is about living well for longer, not simply prolonging life.

DR JOANNA HELCKÉ
DR JOANNA HELCKÉ
specialises in pre/postnatal fitness and has won national awards for her work. She has recently been made an Active Mums Club Ambassador – part of the government Active Together scheme. Joanna is a contributor to magazines, has written articles and material for books and is a public speaker. Most recently, she delivered a talk on postnatal fitness at an NHS workshop for GPs. She is also a qualified vegan retreat chef.
Discover more about working with postnatal clients in this FitPro blog post




